“Do you have a favourite virus?” A strange question, borderline offensive to many. Surely this cannot include potentially fatal viruses such as those that cause flu (influenza), HIV (retroviruses) and cancer (HPV)! As I sneeze twice and blow my nose before I even finish this paragraph, I curse the common cold virus. Doesn’t everybody hate viruses?
But secretly I have a favourite and being an extremely shallow person, it became my favourite upon seeing its 10,000 times amplified image and before knowing what it did…. the bacteriophage “bacteria eater”! This group of viruses includes the T4 phage which looks like an alien nano-machine with its needle-like legs, coiled lower body and diamond-shaped upper body enclosing its genetic material, DNA. Their shape and genetic material (DNA/RNA) varies between phages.
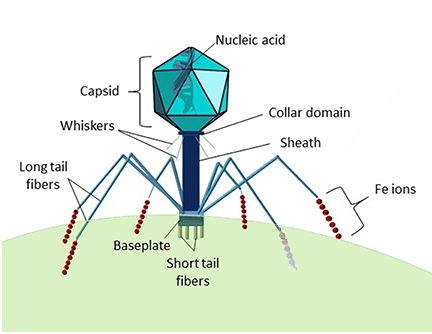
Source: Chelsea Bonnain, Mya Breitbart and Kristen N. Buck via Wikimedia Commons
Each different phage invades specific bacteria in a process known as the lytic cycle. They land on its cell surface and the real similarity with sci-fi begins with a parasite-style alien invasion. The phage injects its genetic material into its target and this integrates with the bacteria’s chromosome. With a mechanism worthy of Mulder and Scully, the bacteria are tricked into making new viruses inside it. Once the new viruses are fully formed, the final phase of the lytic cycle takes place, the lysis of the bacteria which is killed as it bursts open releasing the next alien attack! So these phages have significantly more than good looks!
But could this be a tiny superhero in disguise? The increasing antibiotic resistance by ‘superbugs’ was evident this week with new strains of E. coli infecting thousands in Europe and a new strain of MRSA found in the UK, Denmark and Dublin hospitals. New ways to treat E. coli infection were explored in a New Scientist article on Wednesday. These include therapies aimed at bacteria toxins which have led to kidney damage in the recent E. coli outbreak, vaccinations against specific proteins which allow E. coli to invade the gut and the use of my favourite, bacteriophages, being tested by a UK company to shut down bacterial DNA.
This gave me renewed hope in the potential of bacteriophages. Because antibiotics have been used as the jack of all trades for the last number of years, phage therapy is years behind where it could be. This became obvious when researching for this blog earlier this week. The search terms “bacteriophage”, “phage” and “bacteriophage therapy” led to very few recent articles in major journals (such as Nature, Science, Cell and PNAS) in relation to using phages to treat bacterial infection.
The most recent study I could find was in 2009 in PNAS. Some bacteria such as the new strain of E. coli can’t be treated by most available antibiotics as they react to them by producing more toxin in a reaction called SOS. This study found that the use of phages could enable antibiotic treatment by suppressing the bacteria’s SOS reaction. Ironically, as released at 9pm yesterday by Nature News, the genes in the current E. coli outbreak responsible for the release of toxin are phage genes that have integrated into the bacteria’s chromosome which activate once the SOS reaction begins. So phages also have an extremely dark side!
Before phages could be a viable treatment option, many problems need to be ironed out such as potential immune responses to the virus and the use of different phages for each strain of bacteria which results in high expense rather than the usual broad-spectrum antibiotic model. But perhaps it’s time to end the long-standing chemical vs. bacteria war and let biological warfare begin.
Maybe being shallow isn’t such a bad thing. Looks can kill…. or cure!
Top image: Victor Padilla-Sanchez / Wikimedia Commons


I agree with you that it is time to use bacteriophages for treating bacterial infections; however, I do not agree that there is not enough information available. The problem with phage therapy is that since 1896 when Ernest Hankin first filtered water and reported on antibacterial activity of phages there have been to many false starts – scientist gets grant, scientist isolates new phages and then can’t get more money. Bill Sommers did a review in 2001 or 2003 and if I remember right, he concluded that reviewing English, German and French literature provided enough information to recommend the use of pahge therapy. I think what western countries need to do is accept that Georgia and Poland have become the expert centers for phage therapy and that they should send a few scientists, doctors and regulators for trainig there and then start centers of experimental phage therapy and start using phage therapy when antibiotics fail. Most countries have legal provisions so that this can be done if there is the will to do it. Here is a short handout I use when I give my presentation on the subject of phage therapy:
SUPERBUGS AND BACTERIOPHAGE THERAPY – GETTING BEYOND TRUTHINESS!
(PHAGE THERAPY – ON THE THRESHOLD OF LIFE WHERE CHEMISTRY, BIOLOGY, SCIENCE, RELIGIONS AND FICTION MEET TO CONQUER SUPERBUGS)
Presented by G.W. (Bill) Riedel, PhD, MCIC, Ottawa, at the monthly meeting of the Chemical Institute of Canada, Hawkesbury, Ontario, November 17, 2010.
Paraphrasing Kermit; ‘it is not easy being a superbug’ because for every bacterium, including superbugs, there are a number of viruses that are just waiting to devour them. These viruses are called bacteriophages or simply phages. The tragedy is that we are too venal to deploy these weapons of mass-destruction for bacteria in our efforts to win some battles in the fight with pathogenic bacteria. The science of phage therapy, as the use phages to cure bacterial infections is called, goes back to 1896 when Ernest Hankin, a British bacteriologist, reported on the presence of marked antibacterial activity (against Vibrio cholerae) which he observed in the waters of the Ganges and Jumna rivers in India, and he suggested that an unidentified substance (which passed through fine porcelain filters and was heat labile) was responsible for this phenomenon and for limiting the spread of cholera epidemics. Several other scientists made similar observations; however, in 1917 the French-Canadian microbiologist Felix D’Herelle working at the Pasteur Institute coined the name bacteriophage and experimented with the possibility of phage therapy – he subsequently worked all over world, including Russia, Tbilisi, Georgia, where his efforts survived to this day in the form of a Phage Therapy Center that treats patients from all over the world. The Canadian film: Killer Cure: The Amazing Adventures of Bacteriophage and the book by Thomas Haeusler entitled, Viruses vs. Superbugs, a solution to the antibiotics crisis? ( see http://www.bacteriophagetherapy.info ) attest to d’Herelle’s work and both references are available at Ottawa libraries. According to a letter signed by a former federal health minister phage therapy can be made available legally to Canadians under the Special Access Program of our Food & Drugs Act. In the USA the Food and Drug Administration has amended the US food additive regulations to provide for the safe use of a bacteriophages on ready-to-eat meat against Listeria monocytogenes (see http://www.fda.gov/OHRMS/DOCKETS/98fr/02f-0316-nfr0001.pdf ) and http://www.cfsan.fda.gov/~dms/opabacqa.html ) . The idea that ready-to-eat meat can be treated if contaminated with Listeria bacteria while a doctor could not get a pharmaceutical grade phage therapy product when faced with a patient suffering listeriosis, strikes this author as absurd, especially considering the recent massive recalls of ready-to-eat meat in Canada due to contamination with listeria. Information is available on phage therapy treatment in Georgia , Europe ( http://www.phagetherapycenter.com ) or Poland (http://www.iitd.pan.wroc.pl/en/Phages/ ) or more recently at the Wound Care Center, Lubbock, Texas ( http://www.woundcarecenter.net/ ) .
The presentation will focus on current status of phage therapy around the globe. It is noted that Felix d’Herelle was selected as a laureate of the Canadian Medical Hall of Fame in 2007 for his work with bacteriophages (http://www.cdnmedhall.org/dr-f%C3%A9lix-d%E2%80%99h%C3%A9relle) and it is therefore suggested that Canada should establish ‘The Superbug Victim Felix d’Herelle Memorial Center for Experimental Phage Therapy’ to provide phage therapy to patients when antibiotics fail or when patients are allergic to antibiotics or else Canadians will travel to places where the treatment is available, as did Toronto musician Alfred Gertler in 2001.
Thanks for your reply Bill – interesting food for thought! During my research I did come across some of the work in Georgia but I think for phage therapy to become tested/approved in Europe or the US, scientists from these areas need to do research and receive more support from grant authorities. I found some research that seemed to be promising but as you mentioned their funding was discontinued. However, I agree, I don’t think the information from use of phages in Georgia/Poland should be discounted!